
Creatine monohydrate is the most-studied supplement in sports science, and it works for most people who lift. Five grams a day, any form, any timing. Skip the loading phase; it only accelerates a saturation you'll reach in 4 weeks either way. Expect 1-2 kg of water weight in the first month, and 3-5% more reps at the same load across a handful of compound lifts. That's the return. Everything else (cognition, sarcopenia in older adults) is real but smaller.
What does creatine monohydrate actually do?
The International Society of Sports Nutrition 2017 position stand is the cleanest authoritative summary: creatine monohydrate is effective, safe, and the most well-studied ergogenic aid available ( Kreider et al. 2017 ). The position draws on roughly 700 trials. Headline effect sizes:
- Strength (1RM): ~5-15% increases over typical 6-12 week trials, ranging by lift and training status.
- Power (Wingate test, short sprint): ~5-15% improvements.
- Lean mass: +1-2 kg over 4-12 weeks, above placebo. Most is intramuscular water; a smaller fraction is true hypertrophy driven by higher training volume.
Syrotuik & Bell 2004 (n=34, resistance-trained men) found 5 g/day for 21 days produced 3.7% bench-press 1RM gain vs 1.1% for placebo (p=0.05) ( Syrotuik & Bell 2004, n=34 ). The paper also flagged ~30% of subjects as "non-responders" with low muscle creatine uptake; likely due to baseline dietary creatine (meat eaters saturate less from supplementation).
How does creatine work in muscle?

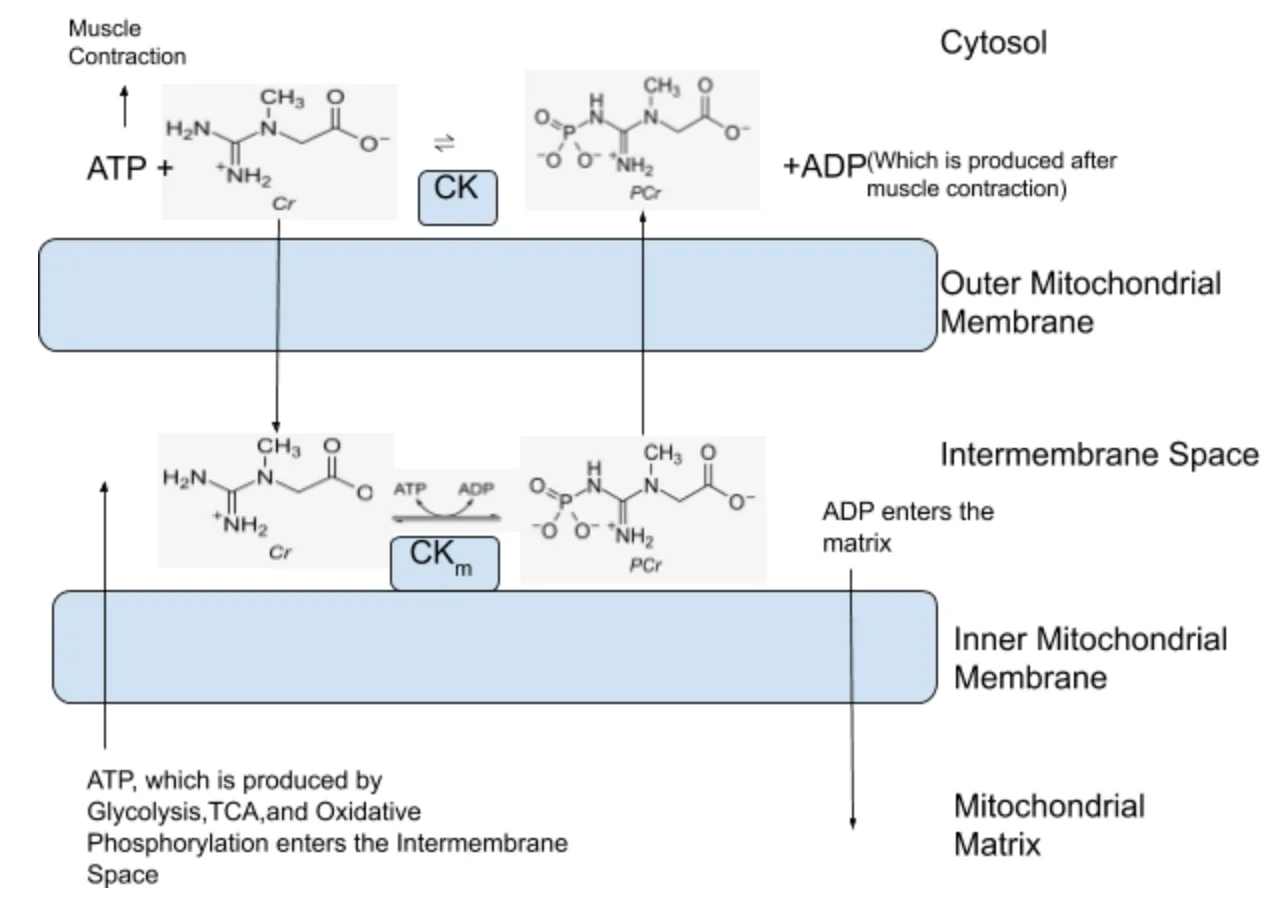
Creatine shuttles phosphate groups onto ADP to regenerate ATP via the phosphocreatine-creatine kinase system. Muscle cells keep ~120-160 mmol/kg dry weight of creatine; supplementation raises this to ~150-160 mmol/kg. The additional phosphocreatine lets you push one or two more reps before your ATP buffer collapses. Over months of training, that "one or two more reps" compounds into meaningful extra volume.
How much creatine should you take daily?
| Phase | Dose | Frequency | Notes |
|---|---|---|---|
| Loading (optional) | 20 g | 4x 5 g/day for 5-7 days | Faster saturation; GI side effects more common. Skip unless you need peak performance in 2 weeks. |
| Maintenance | 5 g | daily | Any form, any timing. Water or juice fine. No cycling needed. |
| Older adults | 5-10 g | daily, split | Some evidence for higher-end dosing past 60 to overcome anabolic resistance. |
Form. Monohydrate is the gold standard. Creatine HCl, buffered (Kre-Alkalyn), ethyl ester, and liquid forms have all been compared head-to-head or in indirect comparison and none outperform monohydrate in meaningful endpoints. Monohydrate is also the cheapest. Don't overpay.
Timing. Doesn't matter. Pre-workout, post-workout, with breakfast, at bedtime. The body's uptake system is not acutely sensitive to timing because the muscle pool saturates over weeks, not hours.
With or without carbs. Insulin elevates creatine transport into muscle slightly, so high-carb co-ingestion can marginally improve uptake. For most adults, this difference is clinically irrelevant.
Cognitive case
Rawson & Venezia 2003 (Amino Acids review) summarized evidence for creatine effects on cognition in older adults with modest positive signals for working memory and reasoning tasks ( Rawson & Venezia 2011 ). Subsequent trials in sleep-deprivation models (university exam weeks, military studies) consistently show preserved reaction time and working memory under conditions that degrade placebo-group performance. Effect sizes are smaller than the muscle literature; the asymmetric bet favors taking it anyway.
Who should not take creatine?
- People with diagnosed kidney disease. Creatine degrades to creatinine; supplementation raises serum creatinine by a cosmetic 0.1-0.3 mg/dL, which can confound eGFR-based monitoring. Clinician conversation first.
- Adolescents in organized sport where creatine may be banned by the governing body. Some high school leagues prohibit it; check.
- Anyone on dialysis or with a known GFR under 60. Talk to a nephrologist.
The supposed risks (dehydration, cramps, hair loss from DHT) are either disproven or based on single low-quality studies. The supposed benefits (treats depression, cures concussion) are overextended.
Cost per dose
A 1 kg tub of plain creatine monohydrate from a reputable brand (Optimum Nutrition, Bulk Supplements, NOW Foods) costs ~$25 in the US, and holds 200 servings. That's $0.12 per serving, or under $4 a month.
The counter-view

Rhonda Patrick is more enthusiastic about creatine's cognitive benefits at higher doses (10-20 g) than the evidence strictly supports; the trials at those doses are small and mostly in clinical populations (TBI, depression). Martin Gibala is more measured: for a person who does not lift, the muscle benefit is small and the cognitive benefit is uncertain. Both are right about their slice.


