
Creatine has been studied in human muscle since 1832, in clinical use since the 1990s, and now sits behind roughly 700 randomized controlled trials, the deepest evidence base of any sports-nutrition compound. The signal is unusually clean: small-to-moderate strength gains, ~1 to 2 kg of additional lean mass, conditional cognitive benefit under stress, and no documented harm in healthy adults at standard doses. This article is a living reference. It will be updated as new trials publish, not as fads cycle through.
What is creatine and where does it come from?
Creatine is a non-essential amino acid derivative. Chemically, it is methylguanidine-acetic acid, with molecular formula C4H9N3O2 and molecular weight 131.13 g/mol. The body holds three relevant pools of it. First, free creatine (~40% of total). Second, phosphocreatine, which is creatine bound to a high-energy phosphate group (~60% of total). Third, creatinine, the spontaneous cyclic breakdown product that gets cleared by the kidneys at roughly 1.6 to 1.7% of the total body pool per day. That cleared creatinine is the basis of the standard kidney-function blood marker, which becomes important in the safety discussion later.
Total body creatine in a 70 kg adult male sits at roughly 120 to 140 g. About 95% lives in skeletal muscle, with the remainder split between brain, heart, kidney, and testes. Muscle creatine concentration runs ~125 mmol/kg dry weight at baseline in mixed-diet adults, with substantial individual variation. Vegetarians cluster lower (~110 mmol/kg) because they get essentially none from food. Carnivores who eat steak daily can sit closer to 140 mmol/kg without supplementing. Hultman's saturation work shows the practical ceiling lands at about 155 to 160 mmol/kg regardless of starting point, which is the biochemical reason supplementation has diminishing returns past 4 weeks ( Hultman, Soderlund, Timmons, Cederblad & Greenhaff 1996 ).
Endogenous synthesis runs about 1 g/day in a healthy adult. The pathway is two-step. Step one happens in kidney and pancreas: arginine + glycine + S-adenosylmethionine yield guanidinoacetate (GAA). Step two happens in liver: GAA gets methylated by guanidinoacetate methyltransferase (GAMT) to produce creatine, which then exports into circulation and gets pulled into target tissues by the SLC6A8 creatine transporter. The pathway is methyl-intensive: ~40% of all SAM-mediated methylation in the body is consumed by creatine synthesis, which is why some authors have speculated that creatine supplementation might spare methyl donors for other reactions like homocysteine clearance. The clinical magnitude of that effect is small but plausible.
Dietary intake covers the other ~1 g/day in mixed-diet adults. Beef, salmon, herring, and pork are the densest sources at roughly 4 to 5 g of creatine per kilogram of raw flesh. A 200 g steak delivers about 1 g. Cooking and processing destroy 10 to 30% of the creatine through conversion to creatinine, which is why the same dose looks different on a label vs in a serving. Lacto-ovo-vegetarians get essentially zero, which is part of why several of the cleanest cognitive RCTs have used vegetarians as their test population: their starting muscle and brain creatine is low enough that supplementation produces a measurable shift.
The compound was first isolated in 1832 by Michel Chevreul. Phosphocreatine was characterized by Cyrus Fiske and Yellapragada Subbarow in 1927. The modern supplement era opened with Roger Harris's 1992 muscle-biopsy work showing that 20 g/day of oral creatine monohydrate raised muscle creatine ~20% in 5 days. Within 4 years it was the dominant ergogenic aid in track and field, and within a decade it was the most-studied substance in sports science.
The point worth holding in mind through the rest of the article: creatine is not a vitamin or a hormone or a stimulant. It is a metabolic intermediate the body already makes and stores in large quantities. Supplementation pushes a saturable pool from ~125 mmol/kg toward its ceiling of ~160 mmol/kg. Everything downstream, the strength gains and the cognitive findings and the aging signals, follows from that simple shift in tissue concentration.
How does the phosphocreatine system actually work?
Skeletal muscle uses three overlapping energy systems during exercise. The phosphagen system covers the first ~10 seconds of all-out work and runs on stored ATP and phosphocreatine. Anaerobic glycolysis covers ~10 seconds to ~2 minutes and runs on muscle glycogen with lactate as a byproduct. Oxidative phosphorylation covers everything beyond that and runs on substrate flux through the mitochondria. Creatine acts on the first system, which is why it shows up in 1RM strength, Wingate sprint output, and rep-out tests at near-maximal load, but not in marathon times.
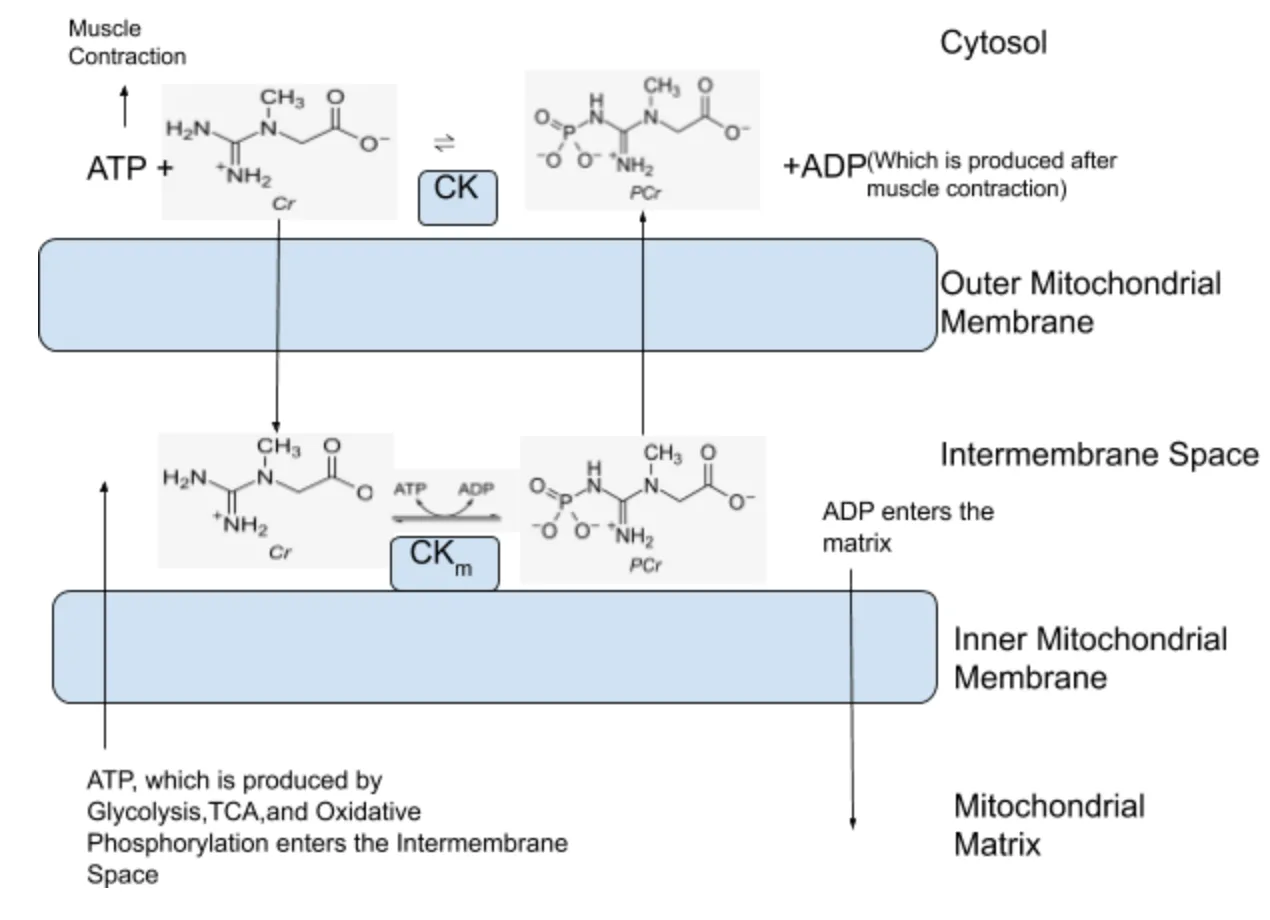
The Lohmann reaction is the central piece. In 1934, Karl Lohmann showed that phosphocreatine donates its high-energy phosphate group to ADP via creatine kinase to regenerate ATP, with a free creatine remaining as the byproduct. The reaction is freely reversible and runs in both directions depending on local ATP/ADP ratios. When ATP demand spikes, as during a heavy set of squats, the reaction runs forward and phosphocreatine acts as an instantaneous ATP buffer. When demand drops, as during rest between sets, the reaction runs backward and phosphocreatine pools refill at the expense of ATP regenerated by oxidative phosphorylation in mitochondria.
Three creatine kinase isoforms do this work in different cellular compartments. Mitochondrial creatine kinase (mtCK) sits on the outer mitochondrial membrane and shuttles phosphate groups from newly-generated ATP onto creatine, producing phosphocreatine that diffuses into the cytosol. Cytosolic creatine kinase (CKM in muscle, CKB in brain) catalyzes the reverse reaction at sites of ATP demand. Sarcomeric creatine kinase (sMtCK) sits at the M-line of the sarcomere and provides on-site ATP regeneration immediately adjacent to myosin ATPase activity. The three-isoform system is essentially a phosphate-shuttling network that decouples mitochondrial ATP production from the location of ATP consumption, with phosphocreatine as the diffusible energy carrier.
ATP regeneration kinetics matter here. Resting muscle ATP concentration is ~5 to 8 mmol/kg. Phosphocreatine at saturation is ~30 mmol/kg. Anaerobic glycolytic capacity is much larger but takes ~5 seconds to spool up to peak rate. During the first 1 to 5 seconds of an all-out sprint or heavy lift, phosphocreatine is the dominant ATP regenerator: it has the fastest kinetics of any energy system in the body. Adding ~20% to that pool through supplementation directly extends the duration and rate of high-output work before anaerobic glycolysis becomes the rate-limiting step.
The fatigue resistance mechanism follows from this. With more phosphocreatine on board, you reach the threshold where ATP production lags ATP demand 1 to 3 seconds later in a maximal effort. In a single set of bench press at 90% 1RM, that translates to 1 to 2 additional reps before bar speed collapses. Across a training block of dozens of such sets per week, the cumulative training volume increase is the proximal driver of the strength and hypertrophy gains observed in long trials. The supplement does not directly cause hypertrophy; it lets you train with marginally higher volume, and the additional volume causes the hypertrophy.
A second-order mechanism involves cell hydration. Creatine is osmotically active; raising intramuscular creatine pulls water in and increases cell volume by an estimated 1 to 3 L over the first month of supplementation. Cell-volume sensing has independently been shown to upregulate protein synthesis and downregulate proteolysis through pathways involving p38 MAPK and FOXO transcription factors. The magnitude of that mechanistic contribution is debated, but most contemporary reviewers ( Kreider et al. 2017 ) consider it a plausible secondary driver alongside the primary phosphocreatine-buffering effect.
For brain tissue, the same biochemistry applies. Cerebral creatine kinase is concentrated in pyramidal neurons of cortex and hippocampus, where ATP demand is high and bursty. Magnetic resonance spectroscopy (MRS) studies show that 5 to 20 g/day of oral creatine raises brain creatine ~5 to 10% in adults, with the largest gains in vegetarians and individuals with low baseline brain creatine on initial scan. This is the mechanistic substrate for the cognitive findings reviewed below: more brain phosphocreatine means more sustainable ATP regeneration during periods of high cognitive load or metabolic stress, with the largest behavioral signal in conditions where ATP supply is constrained (sleep deprivation, hypoxia, vegetarian baseline) ( Roschel, Gualano, Ostojic & Rawson 2021 ).
A subtler mechanistic angle worth noting is the role of creatine in calcium handling and excitation-contraction coupling. Skeletal muscle contraction depends on rapid ATP-driven calcium reuptake by the sarcoplasmic reticulum after each twitch, mediated by SERCA pumps. SERCA activity is sensitive to local ATP/ADP ratio, and any disruption to ATP availability slows calcium reuptake and produces the muscle-specific fatigue pattern of slowed relaxation between contractions. Phosphocreatine, by maintaining local ATP regeneration close to SERCA, indirectly supports calcium clearance and faster relaxation kinetics. This is part of why repeated-sprint protocols benefit from creatine more than single-sprint protocols: the relaxation phase between sprints is partly limited by SERCA-dependent calcium clearance, and that step is exactly where additional phosphocreatine has its largest effect.
The creatine kinase shuttle hypothesis, developed by Saks and colleagues over the past three decades, frames the system as functionally analogous to a battery charging network. Mitochondria charge phosphocreatine; sarcomeric and cytosolic creatine kinases discharge it where ATP is needed. Without the shuttle, free ATP would have to diffuse from mitochondria to myosin, a distance and pathway that diffusion kinetics cannot support during peak demand. The shuttle decouples ATP production from ATP consumption in space and time. Supplementation increases the total charge capacity of this network, which is why the largest behavioral effects appear in efforts that exhaust the system within 5 to 30 seconds. Past 30 seconds, oxidative phosphorylation has caught up with demand and the phosphocreatine reserve is no longer rate-limiting, which is why creatine does not improve marathon time, threshold pace, or VO2max. The biochemistry is dose-specific to the energy system it touches.
How much strength and lean mass does creatine add?

The strength evidence is the deepest part of the creatine literature, with at least four meta-analyses over two decades. Branch 2003 pooled 100 studies and found small-to-moderate effect sizes for body composition and high-intensity performance vs placebo, with the largest gains in untrained subjects and shorter-duration efforts ( Branch 2003 ). Lanhers 2015 and 2017 split the analysis by limb: lower-limb strength gains came in at a weighted mean ES of 0.34 across 60 studies ( Lanhers, Pereira, Naughton, Trousselard, Lesage & Dutheil 2015 ), and upper-limb strength gains converged on a similar effect size in the companion paper ( Lanhers, Pereira, Naughton, Trousselard, Lesage & Dutheil 2017 ). The Kreider 2017 ISSN position stand drew on roughly 700 trials and reached the same conclusion: creatine monohydrate at 3 to 5 g/day after a brief load reliably produces 5 to 15% increases in 1RM, Wingate peak power, and lean mass over 6 to 12 weeks of resistance training ( Kreider et al. 2017 ).
Does creatine monohydrate increase strength and lean mass in adults who train?
| Study | N | Duration | Design | Outcome | Finding |
|---|---|---|---|---|---|
| Branch 2003 meta cite | 100 studies | various | meta-analysis | lean mass + high-intensity performance | small-to-moderate ES (~0.20-0.40) vs placebo |
| Lanhers 2015 lower-limb meta cite | 60 studies | 4-12 wk | meta-analysis | lower-limb 1RM + power | weighted mean ES 0.34 (small-moderate) |
| Lanhers 2017 upper-limb meta cite | 53 studies | 4-12 wk | meta-analysis | upper-limb 1RM + power | comparable upper-limb ES; replicated 2015 finding |
| Kreider 2017 ISSN stand cite | ~700 trials reviewed | varied | position stand | 1RM, Wingate, lean mass | 5-15% strength gains; +1-2 kg lean mass |
| Syrotuik 2004 cite | 34 | 21 d | double-blind RCT | 1RM bench, muscle creatine | +3.7% bench vs +1.1% placebo; ~30% non-responders |
| Chilibeck 2017 elderly meta cite | 22 studies | 7-52 wk | meta-analysis | lean mass + strength in adults >50 | +1.4 kg lean mass and improved 1RM with creatine + RT vs RT alone |
Synthesis Across 4 meta-analyses spanning roughly 200 trials, creatine monohydrate produces small-to-moderate effect-size advantages over placebo on strength (1RM), short-duration high-intensity power (Wingate), and lean mass (~1-2 kg above placebo at 4-12 weeks). The effect is consistent in direction across age groups, training status, and lift selection.
The trial-by-trial pattern is consistent. Volek's 1999 12-week RCT in resistance-trained men (n=19) reported +5.4 kg on bench-press 1RM with creatine vs +1.6 kg with placebo. Becque's 2000 6-week trial in untrained men (n=20) reported +20 kg on biceps 1RM with creatine vs +6 kg with placebo, the larger effect reflecting the untrained baseline. Earnest's 1995 12-week trial reported +20% on 1RM bench in resistance-trained men. Kreider's 1998 28-day trial in football players reported +1.6 kg lean mass with creatine vs +0.4 kg with placebo. The effect sizes vary but the direction does not.
Power and short-duration efforts respond similarly. Wingate peak-power output rises ~5 to 15% on creatine in pooled analysis, with the largest signal in trained subjects performing repeated 30-second sprints. Repeated-sprint protocols (10x6s with 30s rest) consistently show preserved peak power on later sprints in creatine groups, a direct demonstration of the phosphocreatine-resynthesis mechanism. Endurance performance (>2 minute efforts) does not respond, consistent with the phosphagen-system mechanism.
The responder vs non-responder phenomenon is real and well-characterized. Syrotuik & Bell 2004 (n=34) found that ~30% of resistance-trained men showed minimal muscle creatine uptake after standard loading, with corresponding minimal performance gain ( Syrotuik & Bell 2004, n=34 ). Subsequent biopsy work has clarified the mechanism: subjects with high baseline muscle creatine (~150 mmol/kg dry weight) have less room to increase, while subjects with low baseline (~110 mmol/kg) gain more. Vegetarians, with the lowest dietary creatine input, are the population that responds most reliably. Heavy meat-eaters at the upper end of the baseline distribution often respond least.
The lean-mass component deserves a note on water vs true hypertrophy. The first 1 to 2 kg of weight gain in the first 4 weeks is largely intramuscular water from osmotic creatine loading. Beyond that, longer trials (>8 weeks) consistently show the creatine group maintaining a 1 to 2 kg lean-mass lead over placebo, which at that timeframe reflects true muscle hypertrophy driven by the cumulatively higher training volume. DEXA and ultrasound-based muscle thickness measurements tend to converge on the same conclusion: ~70% of the long-term lean-mass advantage is contractile tissue, not water.
Cognitive evidence
The cognitive literature is thinner than the strength literature but the pattern is consistent enough to draw conclusions. Avgerinos 2018 systematically reviewed 6 RCTs of creatine in healthy individuals and found a reliable signal on short-term memory and reasoning tasks under stress, with null results in young, well-rested, well-fed subjects performing baseline cognition ( Avgerinos, Spyrou, Bougioukas & Kapogiannis 2018 ). Roschel 2021 frames the same conclusion mechanistically: brain creatine elevations from supplementation are real on MRS imaging, and the behavioral effects appear in conditions where ATP supply is constrained ( Roschel, Gualano, Ostojic & Rawson 2021 ).
The Rae 2003 vegetarian RCT is one of the cleanest signals in the literature. Forty-five vegetarian adults received 5 g/day creatine or placebo for 6 weeks in a double-blind crossover. Working memory (backward digit span) improved by ~10% on creatine vs placebo, and Raven's progressive matrices, a standard fluid-reasoning test, improved similarly ( Rae, Digney, McEwan & Bates 2003, n=45 ). The choice of vegetarian subjects is methodologically important: their lower baseline brain creatine produced a bigger headroom for change, and the crossover design controlled for individual variation. Rawson & Venezia 2011 reviewed the elderly cognitive literature and reached the same conclusion: modest positive signals for working memory and reasoning in older adults, with the largest effects in subjects with lower baseline cognitive performance ( Rawson & Venezia 2011 ).
The McMorris 2007 sleep-deprivation RCT is the cleanest single-trial demonstration of the stress-cognition pattern. Nineteen subjects received 20 g/day creatine or placebo for 7 days, then performed cognitive testing under 36 hours of acute sleep deprivation. Random number generation, choice reaction time, and several mood measures all degraded substantially in the placebo group across the deprivation window; the creatine group preserved performance close to baseline ( McMorris, Harris, Swain et al. 2006, n=19 ). The mechanistic interpretation lines up: sleep deprivation reduces brain ATP availability, and a higher phosphocreatine buffer offsets the deficit. Subsequent military and shift-work studies have largely replicated this pattern.
Does creatine improve cognition in healthy adults?
| Study | N | Duration | Design | Outcome | Finding |
|---|---|---|---|---|---|
| Rae 2003 vegetarians cite | 45 | 6 wk crossover | double-blind RCT | working memory, Raven's matrices | +~10% backward digit span vs placebo; replicated on Raven's |
| Rawson 2011 review cite | review | various | narrative review | elderly cognition | modest gains in working memory + reasoning, largest in lower-baseline subjects |
| McMorris 2007 sleep-dep cite | 19 | 7 d + 36 h SD | double-blind crossover | RNG, RT, mood under SD | creatine preserved performance vs steep placebo decline |
| Avgerinos 2018 meta cite | 6 RCTs | varied | systematic review | short-term memory + reasoning | reliable benefit under stress (SD, hypoxia); null at baseline in young omnivores |
| Roschel 2021 review cite | review | various | state-of-evidence review | brain creatine + cognition | MRS imaging confirms brain creatine elevations; behavioral signal where ATP is constrained |
| Forbes 2022 brain review cite | review | various | narrative review | cognitive resilience in aging + clinical populations | brain creatine correlates with cognitive resilience under metabolic stress |
Synthesis Across the 6-RCT Avgerinos 2018 meta and the broader Roschel 2021 + Forbes 2022 reviews, creatine reliably improves cognitive performance in vegetarians, older adults, and sleep-deprived or hypoxic subjects. The same dose in young, well-rested omnivores typically produces null results, consistent with the saturation-headroom mechanism.
A useful framing: creatine's cognitive effect is conditional, not generic. The studies that show no benefit are typically run in populations where baseline brain creatine is already near saturation. The studies that show benefit are run in populations where baseline brain creatine is below saturation or where ATP demand temporarily exceeds supply. For a young, well-fed, well-rested omnivore taking creatine purely for cognitive performance, the expected effect at baseline conditions is small. For the same person under exam-week sleep deprivation, the expected effect is larger. This is why the asymmetric bet still favors taking it: 5 g/day costs ~$0.10 and the downside is undetectable, while the upside lands during precisely the periods when cognitive performance matters most.
Brain creatine concentration shifts on supplementation are the mechanistic anchor for all of this. MRS imaging studies put the gain at ~5 to 10% over 4 to 8 weeks of 5 g/day, with the largest gains in subjects with the lowest baseline. Higher-dose protocols (20 g/day) push brain creatine higher faster but plateau in the same range over longer time horizons, because the same saturation logic that governs muscle creatine governs brain creatine. The behavioral correlate is consistent: the populations whose brain creatine moves the most are the populations whose cognitive performance shifts the most.
Aging-specific evidence
Sarcopenia, fall risk, and cognitive decline all become first-order concerns past age 60, and creatine has accumulated enough age-specific data to merit its own section. Chilibeck 2017 meta-analyzed 22 trials of creatine + resistance training in adults averaging ~60 years and found a 1.4 kg lean-mass advantage and improved bench-press and leg-press 1RM vs resistance training alone ( Chilibeck, Kaviani, Candow & Zello 2017 ). The effect size was larger in absolute terms than the average across age groups, which is consistent with the broader pattern that lower-baseline populations have more headroom to gain. Older adults also tend to have lower habitual protein intake and lower baseline muscle creatine, both of which are relevant.
Does creatine help adults over 50 maintain muscle and cognition?
| Study | N | Duration | Design | Outcome | Finding |
|---|---|---|---|---|---|
| Chilibeck 2017 meta cite | 22 studies, mean age >50 | 7-52 wk | meta-analysis | lean mass + 1RM with RT | +1.4 kg lean mass; improved bench/leg-press 1RM vs RT alone |
| Candow 2019 review cite | review | various | narrative review | sarcopenia + [protocol](/tag/protocol/) modifiers | 0.1 g/kg/day + RT identified as operative protocol |
| Forbes 2022 brain cite | review | various | review | cognition in aging + clinical populations | brain creatine correlates with cognitive resilience |
| Rawson 2011 elderly cite | review | various | narrative review | elderly cognition | modest gains in working memory and reasoning |
Synthesis Across the Chilibeck 2017 meta and the Candow 2019 + Forbes 2022 reviews, creatine in older adults reliably adds about 1.4 kg of lean mass when combined with resistance training, and produces modest cognitive gains comparable to those seen in younger trials. The protocol that works mirrors the younger-adult version (3 to 5 g/day) but with stricter adherence to the [resistance-training](/tag/resistance-training/) partner.
The mechanistic case in aging is straightforward. Sarcopenia is partly an anabolic-resistance phenomenon: older muscle requires a higher protein-feeding stimulus to mount the same muscle-protein-synthesis response. Creatine increases training volume by extending high-intensity sets, which in turn increases the mechanical-load stimulus for hypertrophy. The net effect is a partial workaround for anabolic resistance: the older subject can train harder per session, accumulate more total volume per week, and offset some of the age-related decline in MPS sensitivity. Candow 2019 frames this as the operative reason creatine is cost-effective in the over-60 population ( Candow, Forbes, Chilibeck, Cornish, Antonio & Kreider 2019 ).
The fall-risk angle is less direct but worth noting. Several elderly trials have measured functional outcomes alongside lean mass: chair-stand time, timed up-and-go, gait speed, and grip strength. Effect sizes are small (typically a few percent improvement vs control) but consistent in direction, and over a 6 to 12 month horizon they translate to meaningful changes in fall risk and independent-living markers. The mechanism is via the strength gain rather than via creatine acting on balance or reflexes directly: stronger quadriceps and grip mean better recovery from a stumble.
The cognitive-aging case is preliminary but suggestive. Forbes 2022 reviews the brain-creatine literature in older adults and clinical populations and identifies a consistent pattern of cognitive resilience under metabolic stress, mirroring the sleep-deprivation finding in younger adults ( Forbes, Cordingley, Cornish et al. 2022 ). MRS imaging in older adults confirms brain creatine elevations on supplementation, and behavioral testing under conditions of cognitive load (working memory tasks, mental fatigue protocols) tends to favor the creatine arm. Trials in mild cognitive impairment populations are smaller and noisier, but the directional signal is consistent enough that several major aging-research programs are now running larger MCI trials.
A reconciliation is needed for the heterogeneity in elderly trials. Some studies (e.g., Chrusch 2001, n=30) show large effect sizes; others (e.g., Bermon 1998, n=32) show null results. The most parsimonious explanation tracks three variables: (1) whether subjects engaged in adequate resistance training (creatine alone, without training, produces minimal lean-mass gain in older adults); (2) baseline protein intake (subjects below ~1.0 g/kg/day respond less); (3) the dose used relative to body weight (some early trials used 5 g/day in 90 kg subjects, which is below the 0.1 g/kg/day threshold Candow identifies as operative). When these are controlled, elderly-trial effect sizes converge on the younger-adult range.
The practical protocol that comes out of this is unchanged from the younger-adult version: 3 to 5 g/day of creatine monohydrate, taken any time, paired with a resistance-training program of 2 to 3 sessions per week and a protein intake of at least 1.2 g/kg/day. The reason it merits its own section is the higher absolute effect size on functional outcomes that matter more in this population: maintaining the ability to stand up from a chair without using your hands, walk a flight of stairs, and recover from a stumble.
Loading vs maintenance protocols
The loading question is a saturation-kinetics question, and Hultman 1996 settled it three decades ago. Hultman gave one group 20 g/day for 6 days, then dropped to 2 g/day for 30 days. He gave a second group 3 g/day for 28 days. He measured muscle creatine on biopsy at weekly intervals. Both groups reached the same ceiling of ~155 to 160 mmol/kg dry weight: the first group hit it in 6 days, the second hit it in ~28 days ( Hultman, Soderlund, Timmons, Cederblad & Greenhaff 1996 ). The total area-under-the-curve of muscle creatine elevation differs in the first 4 weeks but converges thereafter, and the 28-day-protocol group avoided the GI symptoms that ~20% of the loading-protocol group reported.
The 20 g/day load is typically split into 4x 5 g doses across the day, taken with food. Loading saturates muscle creatine in roughly 5 to 6 days; the daily-3-g protocol takes ~4 weeks to reach the same plateau. Past the plateau, a maintenance dose of 3 to 5 g/day replaces the ~1.6 to 1.7%/day loss to creatinine breakdown. Muscle creatine concentration tracks intake closely: stop supplementing and concentrations return to baseline over ~4 weeks.
The "when is loading worth it" question has a narrow answer. Loading buys ~22 days of earlier saturation. In a competitive athletic context where peak performance is needed in 2 to 3 weeks, loading is the obvious move. In a recreational context where time-to-saturation is irrelevant, loading is the obvious skip: you accept ~22 days of slower onset in exchange for cleaner GI tolerance and simpler dosing. For the over-60 population specifically, the slower 28-day protocol is generally preferred because GI symptoms from loading correlate with body weight and baseline gut health, both of which trend less favorable with age.
Time-to-peak phosphocreatine, as measured on muscle biopsy or MRS, tracks the same kinetics. Loading peaks brain creatine in ~7 days; the daily-3-g protocol peaks brain creatine in ~30 days. Behavioral effects in cognitive trials follow accordingly: loading-protocol cognitive trials see effect sizes within 1 to 2 weeks, while maintenance-only trials typically need 4 to 6 weeks before behavioral changes become reliably measurable.
A common misconception worth addressing: cycling. There is no biochemical rationale for cycling on and off creatine. The creatine transporter (SLC6A8) does not appear to downregulate with chronic supplementation in healthy adults at standard doses, and endogenous synthesis returns to baseline within ~2 weeks of cessation. Long-term users do not develop tolerance in any measurable sense. The 8-weeks-on-2-weeks-off cycling pattern that occasionally surfaces in lifting forums has no published support; it appears to be a holdover from anabolic-steroid cycling logic that does not translate.
The dose-response curve flattens hard above 5 g/day in maintenance. Trials at 10 g/day, 15 g/day, and 20 g/day in maintenance have not consistently produced larger strength or lean-mass effects than 3 to 5 g/day. The exception is the cognitive literature in clinical populations: traumatic brain injury and major depression trials have used 10 to 20 g/day with arguable signals, but the trials are small and the populations are not generalizable. For healthy adults pursuing strength, lean mass, or general cognitive performance, 3 to 5 g/day is the operative dose, and higher doses provide no measurable benefit while increasing GI risk.
For larger individuals (>90 kg), Candow's 0.1 g/kg/day formulation is a reasonable scaling rule: a 110 kg subject ends up at ~11 g/day, a 70 kg subject at ~7 g/day. The evidence base for body-weight-scaled dosing is thinner than for the flat 5 g/day, but the saturation logic supports it: larger subjects have larger total-body creatine pools and need proportionally more to reach ceiling.
A practical loading protocol for athletes who do want it: 5 g of creatine monohydrate, 4 times per day, for 5 to 7 days, taken with food. After day 7, drop to 5 g/day in a single dose for maintenance. Total cost of the load: ~$5 of creatine. Total time investment: trivial. Total gain: muscle creatine saturation in 7 days instead of 28. The reason most authors recommend skipping the load is not that loading is harmful but that the timeline benefit is rarely the binding constraint for recreational users; for a competitive athlete with a meet or a fight in 2 to 3 weeks, the calculation flips and loading becomes the right call.
A further nuance is that some trials in resistance-trained populations have shown comparable strength outcomes between loaded and unloaded protocols at the 4 to 8 week endpoint, even though muscle-creatine saturation kinetics differ. The interpretation is that 4 weeks is enough for the unloaded group to catch up on the metric that matters (muscle creatine concentration), at which point training-volume-driven hypertrophy proceeds at the same rate. This is consistent with the broader pattern that the supplement effect is mediated through saturation, not through any acute pharmacodynamic action: once both groups are saturated, both groups respond identically. Loading is a kinetic shortcut, not a magnitude-changing intervention.
Forms and formulations
The creatine market is a case study in how supplement marketing diverges from supplement evidence. Five forms are commonly sold: monohydrate, hydrochloride (HCl), buffered (Kre-Alkalyn), ethyl ester, and liquid creatine. Monohydrate has roughly 95% of the published evidence. The remaining four together have well under 5%, and the head-to-head trials that exist consistently fail to show advantages for the alternatives.
Creatine monohydrate is the canonical form: a single creatine molecule bound to a single water molecule, ~88% pure creatine by mass. It dissolves at ~14 g/L in water at 20C, which is why a 5 g dose mixes cleanly in 250 mL of liquid without saturating. Bioavailability is essentially complete: orally administered creatine appears in plasma within 1 hour, peaks at 2 to 3 hours, and is taken up by skeletal muscle via SLC6A8 over 4 to 8 hours. Manufacturing cost is low because the synthesis pathway (sarcosine + cyanamide) is mature and high-yielding.
Creatine HCl is creatine bound to hydrochloric acid rather than water, ~78% creatine by mass and ~40x more soluble in water than monohydrate. The marketing claim is that the higher solubility translates to better absorption and lower required doses. The biochemical claim does not survive scrutiny: oral creatine absorption is not solubility-limited at the doses actually used. Monohydrate at 5 g/day already approaches 100% absorption. HCl at 1.5 g/day delivers less total creatine, so even if absorption were marginally better, the muscle-creatine outcome is lower. No published RCT has shown HCl to outperform monohydrate at the muscle-creatine, strength, or lean-mass level.
Buffered creatine (Kre-Alkalyn, pH ~12) is sold on the claim that monohydrate degrades to creatinine in the stomach acid, making buffered forms more bioavailable. Jagim 2012 ran a 28-day head-to-head RCT (n=36) comparing Kre-Alkalyn at 1.5 g/day, Kre-Alkalyn at 5 g/day, and creatine monohydrate at 5 g/day with resistance training ( Jagim, Oliver, Sanchez, Galvan, Fluckey, Riechman, Greenwood, Kelly, Meininger, Rasmussen & Kreider 2012, n=36 ). Muscle creatine content, body composition, and strength outcomes all favored the monohydrate arm modestly or were equivalent. The premise also fails on its own terms: the gastric-degradation rate of creatine monohydrate over a normal transit time is well below 5%, so the bioavailability problem the buffered forms claim to solve does not exist at the magnitude that would matter.
Creatine ethyl ester is creatine modified with an ethyl group, marketed for "enhanced cellular uptake." Spillane 2009 ran a 47-day RCT (n=30) and found that ethyl ester underperformed monohydrate on muscle creatine content and produced higher serum creatinine, indicating greater conversion-to-waste rather than enhanced uptake ( Spillane, Schoch, Cooke, Harvey, Greenwood, Kreider & Willoughby 2009, n=30 ). The compound essentially degrades to creatinine in plasma faster than it gets transported into muscle. It is the worst-performing of the major commercial forms and the easiest to recommend against.
Liquid creatine, sold as a pre-mixed solution, has the same issue as ethyl ester via a different pathway: creatine in aqueous solution slowly degrades to creatinine over weeks, with the rate accelerating at higher temperatures and lower pH. By the time a bottle reaches a consumer, a substantial fraction of the labeled creatine content has converted to creatinine. The cost-per-effective-dose is several times higher than dry-powder monohydrate.
The cost arithmetic settles the question. A 1 kg tub of plain creatine monohydrate from a third-party-tested vendor (Optimum Nutrition, Bulk Supplements, NOW Foods, Thorne) costs ~$25 to $30 in the US and contains ~200 servings of 5 g, or ~$0.12 to $0.15 per serving. The same daily creatine intake from HCl runs ~$0.40 to $0.60 per serving. From buffered creatine, ~$0.50 to $0.80. From ethyl ester or liquid, ~$0.80 to $1.50. Across a year, the difference is $35 to $500 for a daily user, in exchange for either equivalent or worse performance.
What does matter in form selection is third-party purity testing. Plain creatine monohydrate is straightforward to manufacture but easy to contaminate with creatinine, dicyandiamide (a synthesis-pathway intermediate), or heavy metals (chromium, mercury) at low levels. Brands carrying Informed Sport, NSF Certified for Sport, or USP verification have independent batch testing that rules out the major contaminants. Creapure (a German-manufactured monohydrate from AlzChem with documented purity testing) is the gold-standard raw material; many reputable supplement brands source their monohydrate from Creapure and disclose this on the label.
The summary recommendation: monohydrate from a third-party-tested vendor at $25 to $30 per kg. Skip HCl, buffered, ethyl ester, and liquid; the evidence does not support paying for any of them.
A secondary purity consideration is particle size. Micronized creatine monohydrate is mechanically milled to particle sizes of ~5 to 20 microns, compared to ~75 to 100 microns for non-micronized. The smaller particles dissolve faster and stay in suspension longer, which improves the user experience (less gritty residue) without changing bioavailability or efficacy. Micronization adds ~10 to 20% to the per-serving cost. Whether to pay for it is a usability question, not an efficacy question.
Two newer formulations occasionally surface in the marketing literature and deserve brief mention. Creatine magnesium chelate binds creatine to magnesium and is sold on the rationale that magnesium is a cofactor for creatine kinase. The empirical case is weak: head-to-head trials have not shown an advantage over monohydrate, and dietary magnesium intake is the rate-limiting variable for muscle magnesium status, not creatine kinase cofactor availability. Creatine pyruvate combines creatine with pyruvate (a glycolytic intermediate) on the theory that pyruvate provides additional ATP-generation substrate. Trials have produced mixed results, with the most reasonable interpretation being that the pyruvate component contributes minimally and the creatine component performs as expected. Neither formulation has accumulated enough evidence to displace monohydrate as the default.
The dosing volume is also worth a quick note. A 5 g serving of creatine monohydrate is roughly 1 teaspoon by volume. Most monohydrate powders come with a 5 g scoop. Mix in 250 to 500 mL of water, juice, milk, or any beverage and drink within ~30 minutes of mixing (creatine is stable in dry powder for years but degrades to creatinine in solution over hours to days, accelerated by heat and acid). Pre-mixing a daily dose into a water bottle the night before is fine; pre-mixing a week's supply is not.
Safety and side effects
The creatine safety literature is one of the most exhaustively documented in the supplement world, with surveillance datasets running back decades. Kreider 2003 followed 98 NCAA Division I athletes on creatine for 21 months and found no clinically significant differences in liver, kidney, lipid, or hematologic markers vs non-users ( Kreider, Melton, Rasmussen, Greenwood, Lancaster, Cantler, Milnor & Almada 2003, n=98 ). The Kreider 2017 ISSN position stand reviews the broader safety database across hundreds of trials and reaches the same conclusion: in healthy adults at 3 to 5 g/day, no adverse effects on cardiovascular, hepatic, renal, or hormonal markers have been reliably demonstrated ( Kreider et al. 2017 ).
The kidney-function concern deserves the most careful unpacking because it is the most common reason healthy adults reject creatine supplementation. The mechanism that produces the worry is real but cosmetic: ~1.6 to 1.7% of total body creatine spontaneously cyclizes to creatinine each day, gets cleared by glomerular filtration, and shows up on the standard serum creatinine blood test. Supplementing creatine raises body creatine pools, which raises the absolute amount of creatinine produced per day, which raises serum creatinine by ~0.1 to 0.3 mg/dL. This is an artifact, not a kidney injury: the kidneys are filtering more creatinine because more is being produced, not because filtration capacity has dropped ( Poortmans & Francaux 2000 ).
The clinical resolution is straightforward in the research literature. Cystatin C is a small protein produced at constant rate by all nucleated cells and cleared by glomerular filtration; unlike creatinine, it is not affected by muscle mass or creatine intake. Cystatin-C-based eGFR is the gold-standard kidney-function measurement when creatinine is confounded. Gualano 2008 ran a 12-week creatine RCT in healthy resistance-trained men (n=18) and measured cystatin-C-based GFR alongside creatinine-based GFR; the creatinine-based GFR rose mildly (the artifact), while the cystatin-C-based GFR was unchanged (the actual kidney function) ( Gualano, Ugrinowitsch, Novaes, Artioli, Shimizu, Seguro, Harris & Lancha 2008, n=18 ). The same pattern has been replicated in older adults, athletes, and clinical populations. Healthy kidneys handle the additional creatinine load without measurable functional change.
This does not extend to populations with diagnosed kidney disease. In stage 3+ chronic kidney disease, the kidneys are already filtering near capacity, and the additional creatinine load from supplementation could plausibly be problematic. Anyone with a diagnosed eGFR under 60 mL/min/1.73 m^2 should discuss creatine with a nephrologist before starting. The same principle applies on a smaller scale to people taking medications that affect kidney function: ACE inhibitors at high dose, NSAIDs at chronic high dose, certain antibiotics. These are all clinician-conversation cases, not automatic exclusions.
GI tolerance is the other commonly reported side effect, almost always associated with high single doses. The 20 g/day loading protocol, taken as 4 doses of 5 g, produces mild GI symptoms in ~10 to 20% of subjects: bloating, diarrhea, nausea. The mechanism is osmotic: a single 5 g dose raises gut-lumen osmolarity transiently, drawing water into the lumen. Splitting the dose into smaller portions (2 g x 4 to 5 per day) or skipping the load entirely resolves the issue in essentially all cases. At maintenance doses of 3 to 5 g/day, GI symptoms are rare.
The hair-loss claim deserves specific attention because it is common and the underlying evidence is thin. The entire claim traces back to a single 2009 RCT: Van der Merwe 2009 (n=20 college rugby players) reported that 7 days of 25 g/day creatine loading followed by 14 days of 5 g/day maintenance raised the dihydrotestosterone-to-testosterone ratio by ~22% ( van der Merwe, Brooks & Myburgh 2009, n=20 ). The trial measured serum DHT, not hair density, hair-follicle count, or any direct hair outcome. It has never been replicated, and several subsequent RCTs measuring testosterone and DHT on creatine supplementation have not found the same effect. The chain of reasoning required to get from "single underpowered trial showing serum DHT elevation" to "creatine causes hair loss" requires multiple unsupported steps. The fair statement of the current evidence: the existing data are insufficient to support the claim that creatine accelerates androgenetic alopecia. If you are already on finasteride or have a strong family history of male-pattern baldness, the precautionary case against creatine remains weak and undocumented.
Water retention is real but smaller and shorter-lived than commonly stated. The first 4 weeks of supplementation produce ~1 to 2 kg of intracellular water gain, primarily inside skeletal muscle cells. This is not the puffy subcutaneous water retention associated with high-sodium diets or certain medications; it is intramuscular and looks like increased muscle fullness rather than facial bloating. Past the saturation phase, water retention does not progress: total body water stabilizes at the new equilibrium and does not continue to climb.
The list of conditions that warrant clinician conversation before starting: diagnosed kidney disease (stage 3+ CKD), diagnosed liver disease, pregnancy or lactation (where the safety database is thin rather than negative), and concurrent use of nephrotoxic medications. For everyone else in the healthy adult population, the long-term safety record is among the best of any supplement studied at this depth.
Stacking and timing
The stacking literature is more anecdotal than the strength literature, but a few combinations have enough trial coverage to draw modest conclusions. The clearest synergy is creatine + protein post-workout. Cribb 2007 (n=32 resistance-trained men, 10 weeks) compared a protein + creatine + glucose post-workout supplement to protein-only and found ~2 kg additional lean-mass gain in the combined arm vs the protein-only arm. The mechanism is plausible: insulin from glucose acutely increases creatine transporter activity, modestly improving muscle creatine uptake during the peri-workout window. The effect size is small and the trial population is narrow, so the practical recommendation is "if you are already taking protein post-workout, add creatine to it" rather than "creatine without post-workout protein is suboptimal."
Timing matters less than the marketing implies. For an established user at saturation, total daily intake is the only variable that matters for muscle creatine concentration. The transporter is not acutely sensitive to time-of-day, fed vs fasted state, or peri-workout proximity. Pre-workout creatine and post-workout creatine produce identical 12-week strength outcomes in head-to-head comparisons. The "creatine works best post-workout" claim in supplement marketing is overstated: the difference, where measurable at all, is small compared to the variance in individual response.
For new users still loading or building toward saturation, peri-workout timing has a slightly stronger rationale via the insulin-transporter mechanism, but the magnitude is again small. The practical advice is to take creatine at whatever time of day produces the best adherence, which is the variable that actually predicts long-term muscle creatine concentration.
The caffeine antagonism debate is one of the longer-running side controversies in the literature. Vandenberghe 1996 (n=9 crossover) reported that 5 mg/kg/day caffeine consumed during a 6-day creatine load blunted the performance gains seen in the creatine-alone arm ( Vandenberghe, Gillis, Van Leemputte, Van Hecke, Vanstapel & Hespel 1996 ). The claim entered the supplement-industry consciousness as a categorical "do not take creatine with caffeine." The follow-up trials largely failed to replicate the antagonism in strength, power, or muscle-creatine outcomes when caffeine was taken acutely (e.g., 1 hour pre-workout) rather than chronically alongside creatine loading. Several pre-workout supplements containing both creatine and caffeine have produced normal creatine performance gains in their own RCTs. The current best estimate: chronic high-dose caffeine (>5 mg/kg/day) consumed simultaneously with creatine loading may modestly blunt loading kinetics, but acute pre-workout caffeine in established creatine users produces no detectable interference. The Vandenberghe finding is a real signal that has been overgeneralized.
Beta-alanine + creatine is a stack with reasonable empirical support. Beta-alanine raises muscle carnosine, which buffers intramuscular pH during anaerobic glycolysis. Creatine extends the phosphagen-system buffer for the first 5 to 10 seconds of work; beta-alanine extends the glycolytic-system buffer for the 30-second to 2-minute window. The two compounds operate on adjacent energy systems with minimal overlap, and combined trials have shown additive effects on repeated-sprint and high-rep work. The stack is most useful for athletes whose competitive demand sits in the 30-second to 2-minute range (rowing, middle-distance running, MMA round work).
Carbohydrate co-ingestion modestly improves creatine uptake during loading. Steenge 1998 showed that adding ~95 g carbohydrate to a 5 g creatine dose raised muscle creatine retention ~15% over creatine alone, mediated by insulin-driven creatine transporter upregulation. The effect size shrinks substantially in the maintenance phase: at saturation, additional uptake is constrained by the muscle-creatine ceiling, not by transporter activity. For most users, the practical translation is "take creatine with food if convenient, but do not engineer carbohydrate spikes around it."
HMB (beta-hydroxy-beta-methylbutyrate) and creatine have been combined in older-adult and untrained-adult trials with modest additive signals on lean mass, but the HMB evidence base is much thinner than the creatine evidence base, and the cost-per-effect of HMB is substantially higher. The stacking case is weak: take creatine, lift, and decide separately whether HMB warrants its own line item.
The negative stack worth noting: creatine + diuretics, which is a stack that elite endurance athletes occasionally use to manage water-weight gain during creatine supplementation. The combination is risky: creatine pulls water intracellularly while diuretics pull water from extracellular spaces, and the resulting fluid imbalance can compromise thermoregulation during hot-weather training. There are case reports of dehydration and rhabdomyolysis in this combination at high dose. For recreational users this is not a relevant scenario, but the mechanism is worth understanding.
Creatine + caffeine, despite the Vandenberghe controversy, is the most common real-world stack: pre-workout supplements pair the two routinely, and the empirical performance data on those products has not produced a categorical antagonism signal. The conservative interpretation is that simultaneous chronic high-dose caffeine during loading may modestly slow saturation kinetics, but the practical effect on a user already at saturation is small enough to be undetectable in most trials. If you are a heavy daily caffeine consumer (>400 mg/day) and concerned about the interaction, separating creatine from caffeine intake by 2 to 3 hours is a low-cost hedge that preserves both. For most users, this level of attention to timing is unnecessary.
Creatine + alcohol is worth a brief mechanism note. Acute alcohol consumption suppresses muscle protein synthesis for ~24 hours after intake, which can blunt resistance-training adaptation independent of creatine. Alcohol also acts as a mild diuretic, which can interact with creatine's intracellular water-loading effect. The net result is that creatine plus heavy drinking does not undo the creatine effect (the muscle creatine pool is robust to acute alcohol) but the strength and lean-mass gains the protocol is meant to produce will be partially offset by the alcohol-driven MPS suppression. Creatine cannot rescue training gains from chronic heavy drinking; protein and creatine and lifting are all downstream of total alcohol intake.
A timing question that recurs is fasted-state vs fed-state ingestion. The mechanistic case for fed-state ingestion (insulin-driven creatine transporter upregulation) applies most cleanly during loading, when uptake is the rate-limiting step. At maintenance, when the muscle pool is saturated, the transporter is not the bottleneck and fed vs fasted ingestion produces equivalent outcomes. For users on intermittent fasting protocols who want to take creatine in the fasted window, the practical answer is that it works fine: a 5 g dose of creatine monohydrate has no meaningful caloric content and does not break a fast in any biologically relevant sense.
Stacking creatine into a peri-workout shake with whey protein and a carbohydrate source (~30 g whey + ~30 g carbohydrate + 5 g creatine) is the most evidence-based of the post-workout stacks. The Cribb 2007 trial and several subsequent replications have shown small but reliable additional lean-mass gains for the combined stack vs the protein-only stack. The effect size is small and the practical translation is "if you already make a post-workout shake, add creatine to it" rather than "engineer your training schedule around the post-workout window."
Practical FAQ and verdict
Do I need to cycle creatine? No. The transporter does not desensitize at standard doses, and there is no published support for cycling. Stay on it.
Does creatine cause hair loss? The current evidence is insufficient to support the claim. The chain of reasoning rests on a single 2009 trial (n=20) measuring serum DHT, not hair density, that has never been replicated. If you are already on finasteride for hair loss, creatine is not contraindicated.
Should I worry about kidney function? No, in healthy adults. Serum creatinine rises ~0.1 to 0.3 mg/dL on supplementation as a creatine-to-creatinine breakdown artifact, but cystatin-C-based GFR is unchanged in published trials. If you have diagnosed CKD or are on nephrotoxic medications, talk to a clinician.
Monohydrate vs HCl vs buffered vs ester? Monohydrate. Five RCTs, including Jagim 2012 (n=36) for buffered and Spillane 2009 (n=30) for ester, have failed to show advantages for the alternative forms, while monohydrate is 3 to 10x cheaper.
Loading or no loading? Loading buys ~22 days of earlier saturation in exchange for higher GI risk and more complicated dosing. If you do not need peak performance in the next 2 weeks, skip the load and take 5 g/day for 4 weeks to reach the same plateau.
Best time of day to take creatine? Whatever produces the best adherence. For established users at saturation, timing is irrelevant; daily total intake is the variable that matters.
Do I need to take a break for liver or kidney recovery? No. Twenty-one-month surveillance data in NCAA athletes shows no liver, kidney, or lipid markers shifting outside reference ranges ( Kreider, Melton, Rasmussen, Greenwood, Lancaster, Cantler, Milnor & Almada 2003, n=98 ). The "needs a break" framing is borrowed from anabolic-steroid logic and does not apply.
Does creatine work for vegetarians better than carnivores? Yes, on average. Vegetarians have lower baseline muscle and brain creatine and more headroom to gain, which translates to slightly larger effect sizes on both strength and cognition. Carnivores still respond, just from a higher starting baseline.
Will creatine make me bloated or puffy? The first month produces 1 to 2 kg of intracellular water gain inside muscle cells. This presents as fuller-looking muscles, not facial puffiness or subcutaneous bloating. Past 4 weeks, no further water retention.
Is creatine safe for adolescents? The pediatric safety database is smaller than the adult database but largely positive. The main practical concern is sport-governing-body rules: some high school and youth leagues prohibit it. Check first.
Creatine for people who do not lift? The strength benefit requires resistance training to materialize. The cognitive and aging benefits do not require lifting and accrue independently. For a sedentary older adult, creatine + walking + adequate protein still produces lean-mass and functional gains, just smaller than the same protocol with resistance training added.
How long until I notice the effect? Strength and rep-out tests start showing changes at 2 to 4 weeks for loading-protocol users, 4 to 8 weeks for maintenance-only users. Cognitive effects in vegetarians and older adults appear on a similar timeline. Subjective changes in muscle fullness appear within 1 to 2 weeks.
What does a clinician dissent look like? Stuart Phillips, a respected protein and resistance-training researcher, has argued that the marginal benefit of creatine in well-fed, well-trained adults is small enough that the evidence-effort-payoff favors prioritizing protein and training quality first. The position is reasonable; creatine is the addition after the basics are in place, not a substitute for them. The case for adding it remains strong because the cost is so low and the downside risk is so small.


